
KJIPUKTUK (Halifax) – How prepared has our health care system been for the demands of the current COVID-19 pandemic? With hospitals worried about having enough ventilators and personal protective equipment and the angels of death haunting seniors’ homes, it’s time to go back to the future.
In November 2007, a few years after the 2003 SARS crisis Judy Haiven and I published “Health Care Strikes: ‘Pulling the Red Cord.’” with the Canadian Centre for Policy Alternatives and it made some observations and predictions about the ability of our health care system to cope with catastrophes. With another pandemic upon us, let’s reflect upon that report
What was merely informed speculation at the time has turned out to be frighteningly accurate with the passage of time.
We built the following argument, which is only more pertinent today:
From the late 1970s, faced with increasing competition from the Japanese, North American manufacturers began adopting a strategy called variously “management-by-stress,” “continuous improvement,” or “lean production”.
The strategy called for a relentless diminution of “waste” in workplaces just short of breakdowns occurring. Factory management wanted to see just how close production could come to failing without failing completely.
The Japanese system relied on engineers, but also upon production workers reporting and acting. The “Andon” or signature indicators warned of problems. One of the best-known of these signals were three lights. Green signified that the system was proceeding without problems. Red indicated that production had stopped due to problems. In lean production, the predominance of either of these conditions is not desired. Too much green and the system is not lean enough. Too much red means there are not enough resources. It is the yellow light (or yellow condition) that is prized.
Production line workers had some control over the line and could pull the red cord to stop production for corrective adjustment in technology or personnel.
We argued that the principles in manufacturing drifted inevitably to the public sector:
The gospel of lean has expanded well beyond private-sector auto manufacturing. It has migrated into our public services. At first so popular in manufacturing, lean was hard to resist in the service sector, fuelled by consultants, especially in the profit-making, efficiency-seeking private hospitals in the US.
In the public sector, it became known as the “New Public Management.” As Canada moved into the fiscal panic of the [early] 1990s, the model was irresistible to our public sector. The public health care system, too, succumbed to the relentless “cult of efficiency.” And even acute care institutions adopted the general approach of management-by-stress.”
We further argued that the veneration of productivity at-all-costs might be acceptable in automobile manufacturing, but it was wilfully reckless in health care, where cuts could put populations in danger during periods of unexpected and catastrophic stress. While Japanese autoworkers in a classical Kaizen production line had the power to “pull the red cord”, health care workers have no such power and that they, their patients and the health care system were helpless. Health care simply cannot operate with minimum capacity.
It turns out that truth is stranger than knowledgeable conjecture. In the “Red Cord” report, we were using the concept of “Lean” as a metaphor to make enforced emaciation of health care more understandable. We never thought that any Canadian health authority would have the chutzpah to adopt not only the substance, but the nomenclature as well.
But that is precisely what the Saskatchewan government did in 2011. Lean had been introduced in Britain’s National Health Service in 2008 and the buzz had worked its way across the ocean. Saskatchewan hired “John Black and Associates: Lean Healthcare Consultants” and paid out between $44 and $50 million to realize the testament of Black’s 2008 book The Toyota Way To Healthcare Excellence: Increase Efficiency and Improve Quality With Lean (published at least a year after our “Red Cord” report.)
The Saskatchewan Health Authority’s own web pages (last modified in May 2017 but still “live”) continue to extoll the virtues of Lean:
In health care, Lean is a patient-centred approach that helps employees, physicians, patients and families work together to find ways of improving processes and eliminating waste so that everyone receives reliable, safe, timely, high-quality health care. When waste, (such as patient waits, health test duplication or sta time searching for supplies) is eliminated, costs are often reduced.
Lean first began in the manufacturing industry but has since been successfully applied to many other sectors including health care. Lean focuses on driving waste out of processes, and continually asks whether a product or service has value in the eyes of the end-user. Saskatchewan is among the first provinces in Canada to apply Lean concepts and tools across its entire health system.
https://www.saskatoonhealthregion.ca/about/Our-Plan/Pages/Lean.aspx accessed 3 April, 2020
The website’s “Better Every Day Glossary of Terms” is replete with continuous improvement argot, including many Japanese terms like “Gemba” (the workplace), and “Andon” (the signal, like the red light, indicating problems.) One of the most controversial aspects of the project was the importation of Japanese “sensei”s (teachers) at $3,500 a day.
Thomas Rotter, of Queen’s University’s Health Quality Programs and formerly University of Saskatchewan Chair in Health Quality Improvement Sciences claimed “They are still hiding the big failures in Lean.”
Rotter’s research reveals that 75 per cent of nurses and 42 per cent of other health professionals reported some or substantial workload increases, while 17 per cent of nurses and 48 per cent of other health professionals claimed Lean had no impact.
Rotter’s report suggests “Little has been documented about the failed attempts or barriers to implementation, adoption and sustainability of Lean principles in health care.”
Even by the standards of cost-saving, the Saskatchewan Lean project was problematic. The provincial auditor general reported that there was no evidence the Lean programs produced better service, or value for the money spent. Indeed, the government was not keeping track of results. The A-G stated, “They’re unable to show us whether or not Lean is achieving what they’re hoping it’s achieving.” The auditor pointed to 100s of Lean events and 5,000 days of staff time expended on the project, with no results recorded.
A report in the International Journal for Quality Health Care calculated that for every dollar saved by Lean, Saskatchewan spent $1,511. The article also claimed that “Outcomes reported a statistically significant negative effect of Lean on nurse engagement, usefulness, patient care, time for patient care, workplace issues, availability of supplies, workload stress, and patient safety.”
An analysis of the academic literature concluded that “Lean interventions have: (i) no statistically significant association with patient satisfaction and health outcomes; (ii) a negative association with financial costs and worker satisfaction and (iii) potential, yet inconsistent, benefits on process outcomes like patient flow and safety.”
Why did Saskatchewan fall so heavily for the promises of the Lean guru? A now classic cultural trope can be found in The Simpsons episode on the monorail.
A telling and resonant anecdote sums up the problem with Lean. It is recounted by a group of Saskatchewan researchers. In pre-Lean days, continuing care assistants working in a home care institution would meet for a “huddle” or case conference every day to discuss the roster of their patients/clients and their needs before going on their rounds. Armed with information and recommendations, they were better able to improve care. But the “huddle” practice could not withstand the scrutiny of the Lean process. It was deemed a wasteful exercise and fell victim. Thus effectiveness in health care gave way to efficiency. This is one of the most devastating critiques of Lean.
What could $50 million have been spent on, if not on Lean? How about the following preparatory items for a pandemic, as an example?
- 1000 hospital beds, plus
- 1000 ventilators, plus
- 50,000 N95 face masks
- Employment of 10 medical residents for 3 years, plus
- Employment of 25 RNs for 3 years, plus
- Employment of 50 LPNs for 3 years, plus
- Employment of 10 registered respiratory therapists for 3 years, plus
- An MRI machine, for good measure
So controversial became the Lean venture that the Saskatchewan government ended its contract with Black and Associates in 2015.
Lest we rely too heavily on the Saskatchewan example, the Lean adventure in that province may be nothing but a hilarious sideshow of the main event across the country, which is the dropping of the capacity of the health care system everywhere to deal with shocks like SARS and COVID-19. Whether Canadian governments were as bold and imprudent as Saskatchewan to buy into the rigmarole of Lean, hook, line and sinker, or not, they have all been following the same trajectory, which is to say, impoverishing workers and the public sphere in order to shovel money at the rich.
Wealth, expressed as real GDP per capita, has grown by almost 50% since 1975. In other words, on average Canada is half again as rich as it was 45 years ago. But real incomes of the sellers of labour have hardly budged. Nearly all of that increase in wealth has been captured by owners of capital. In the name of austerity, public services have been cut back drastically. If a system runs close to emergency at the best of times, how can it respond to a real emergency? An emergency like COVID-19?
One indicator of capacity is hospital beds per 1000 population. The World Health Organization recommends 5.0. The current OECD average is 4.8. As of 2017, Canada stood almost last at 2.52 compared to Japan at 13.05, South Korea at 12.27, France at 5.8 and Norway at 3.60. Nova Scotia has 2.7 and, after Saskatchewan’s Lean venture, that province has only 2.2 beds per 1000.
Another indicator of capacity is the proportion of total healthcare spending disbursed for hospitals. From a high of 44.7% in 1975, Canada has dropped steadily to 26.9% in 2019.
Another indicator of capacity of the health care system is the availability of face masks. Of current the COVID-19 crisis, the perceptive Stephen Kimber writes:
…we’re at the tail-wagged end of a worldwide shortage of masks.
And that’s because almost no one in charge of our modern, sophisticated just-in-time, ready-as-needed, don’t-worry-be-happy global supply chains paid attention to the worst-case scenarios that were, in fact, being gamed out with frightening accuracy for years in private think tanks and in the far forgotten corners of government bureaucracies.
Stockpiles? Don’t worry. We’re covered. Until we weren’t.
Now those supply chains have been frayed and fractured by the unprecedented pressures of the current crisis.
https://www.halifaxexaminer.ca/featured/mask-mask-whos-got-the-mask-and-other-global-games-from-the-coronavirus-killing-fields
The stats for long-term care are equally alarming. As the proportion of seniors in the population grows, the number of nursing home beds in Canada per 1000 population aged 65+ has dropped from 41.2 in 2005 to 26.5 in 2014. That number dropped in other countries as well. But in 2014, Norway still far outdid Canada at 49.5 beds, Sweden at 46.4 and the US at 36.6.
The 2003 SARS outbreak in Toronto, where forty-four people, including several health care personnel, died gives us an example of a vulnerable health care system subjected to unexpected stresses. While the disaster could not have been foreseen or avoided, the fact that it became so calamitous can be in large part attributed to the lack of back-up resources.
Mr. Justice Campbell wrote a report on the crisis and concluded, “More financial and professional resources are needed, otherwise all the legislative changes and programme reforms will prove to be nothing but empty promises. The test of the government’s commitment will come when the time arrives for the heavy expenditures required to bring our public health protection up to a reasonable standard.”
One of those testifying before the Campbell Commission was Dr. Bernadette Stringer, an epidemiologist from Western University and former emergency and critical care nurse. Stringer argued that under conditions like SARS, health care workers under stress are less effective than they could be. The well-being of patients is intimately connected to that of their caregivers:
When a hospital is made safer and healthier for the people who work there, it also becomes a better facility for the people who are being treated or who are recovering there. The health and safety of patients and healthcare personnel are two sides of the same coin.
Furthermore, other industries crucially concerned with the care and safety of clients often succeed, not through an obsession with leanness, but precisely its opposite.
It has long been recognized in other sectors, such as the aviation industry, that interventions targeting the system, that is, interventions such as reducing workload or increasing the amount of time off between work shifts to decrease fatigue or creating standardized procedures are the most effective ways of addressing medical errors. These interventions make the aviation industry safer and healthier for air crews and passengers. There is every reason to believe that similar approaches in the healthcare industry would make it safer and healthier for workers and their patients. In summary, health care should not be run under a system of “management-by-stress.” It is totally inappropriate where human lives are at stake, where the unexpected is normal and where the technology of service delivery is rapidly changing.
In 2006, three years after SARS, leading Canadian healthcare authorities (including now Chief Public Health Officer of Canada Theresa Tam) published a report on preparedness for a similar contagion. A federal audit in 2010, after the H1N1 outbreak noted problems with management of the country’s stockpile of emergency medical equipment. A 2018 evaluation of the 2008 H1N1 swine flu contagion discussed ventilator shortages, and a study by a group of international scientists a year later questioned whether countries like Canada would be ready for a pandemic.
Responding last April 9 to news of the 2006 report, Canadian Medical Association President Sandy Buchman opined: ““I am trying to understand the government’s response today because I think everyone was caught flat-footed. The front line is telling us over and over that they are not prepared, and they are scared. We are hearing it from everywhere.”
A simple but elegant little chart produced near the beginning of the COVID-19 pandemic has brilliantly alerted us to the importance of social distancing. Using easily understood concepts, “flattening the curve” warns us that we must avoid the exponential growth of infection cases lest the capacity of even modern health care systems be overwhelmed, as has happened in countries like Italy.
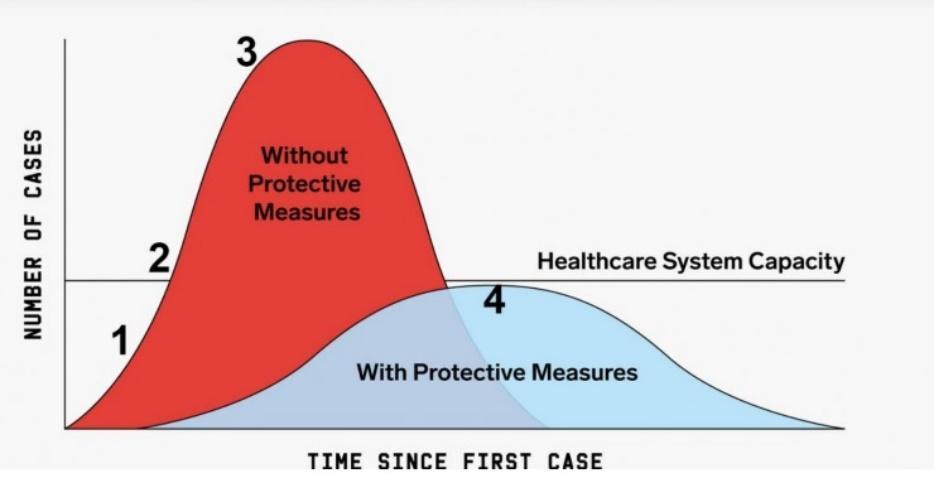
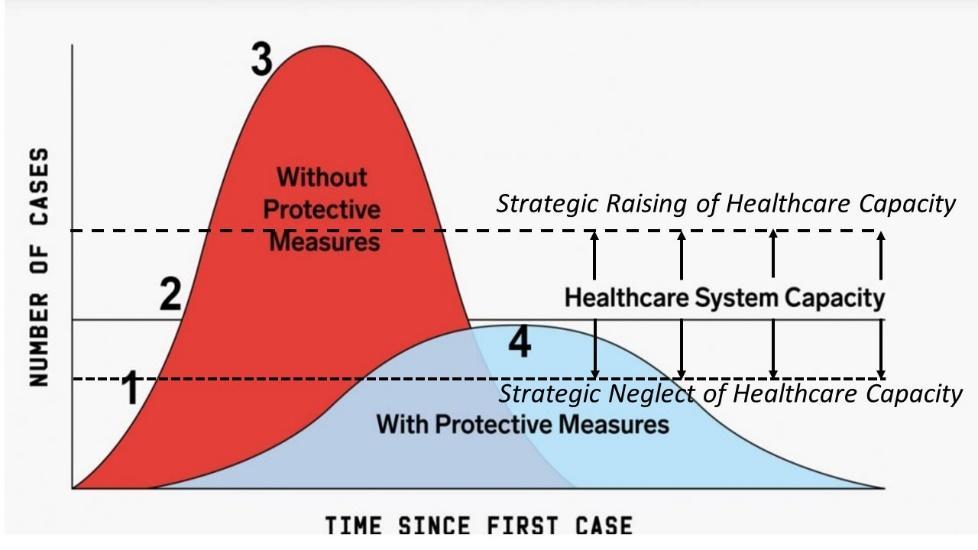
But a huge problem with the “flattening the curve” chart is the way it treats “healthcare system capacity” as a constant. It ignores the reality that system capacity is a mutable phenomenon. As shown above, over the past half century, capacity has been in political play, and not in a good way.
The graph needs to be altered, to bring capacity back into the picture (see below): Flattening the curve is crucial, but so is improving capacity. Let’s hope we finally learn both lessons.
Click here for a fully footnoted version of this article.
Larry Haiven is professor emeritus at Saint Mary’s University, on the steering committee of Equity Watch and a research associate of the Canadian Centre for Policy Alternatives – Nova Scotia.
With a special thanks to our generous donors who make publication of the Nova Scotia Advocate possible.
Subscribe to the Nova Scotia Advocate weekly digest and never miss an article again. It’s free!



This is so good. Thank you to Larry. I work at the IWK and Lean is fully entrenched here. I have heard from a nurse who told me she lost a job because she wasn’t enthusiastic enough about Lean when asked about it in an interview. This is the feedback she received when she asked for a review of why she lost out in the interview process.
The ideology of Lean is in keeping with neoliberalism where the public sector is just always starved of funds so that less taxes have to be spent on essential things like public services like health care. The really sad part of this is that people have been very successfully brainwashed by the captains of industry and their servants in government to believe that tax cuts and lower taxes and less spending is somehow a good thing, even as the public consistently insists that they love their health care system.